You didn’t expect to be back here.
Not after the first round of therapy. Not after the promises. Not after the relief you felt when things seemed steady.
And yet—something feels off again. Or maybe it’s not subtle at all. Maybe it’s obvious. The mood swings. The isolation. The lies that don’t quite hold together.
As a clinician who works closely with families, I want to say something gently but clearly:
Your love did not cause this.
And your exhaustion makes sense.
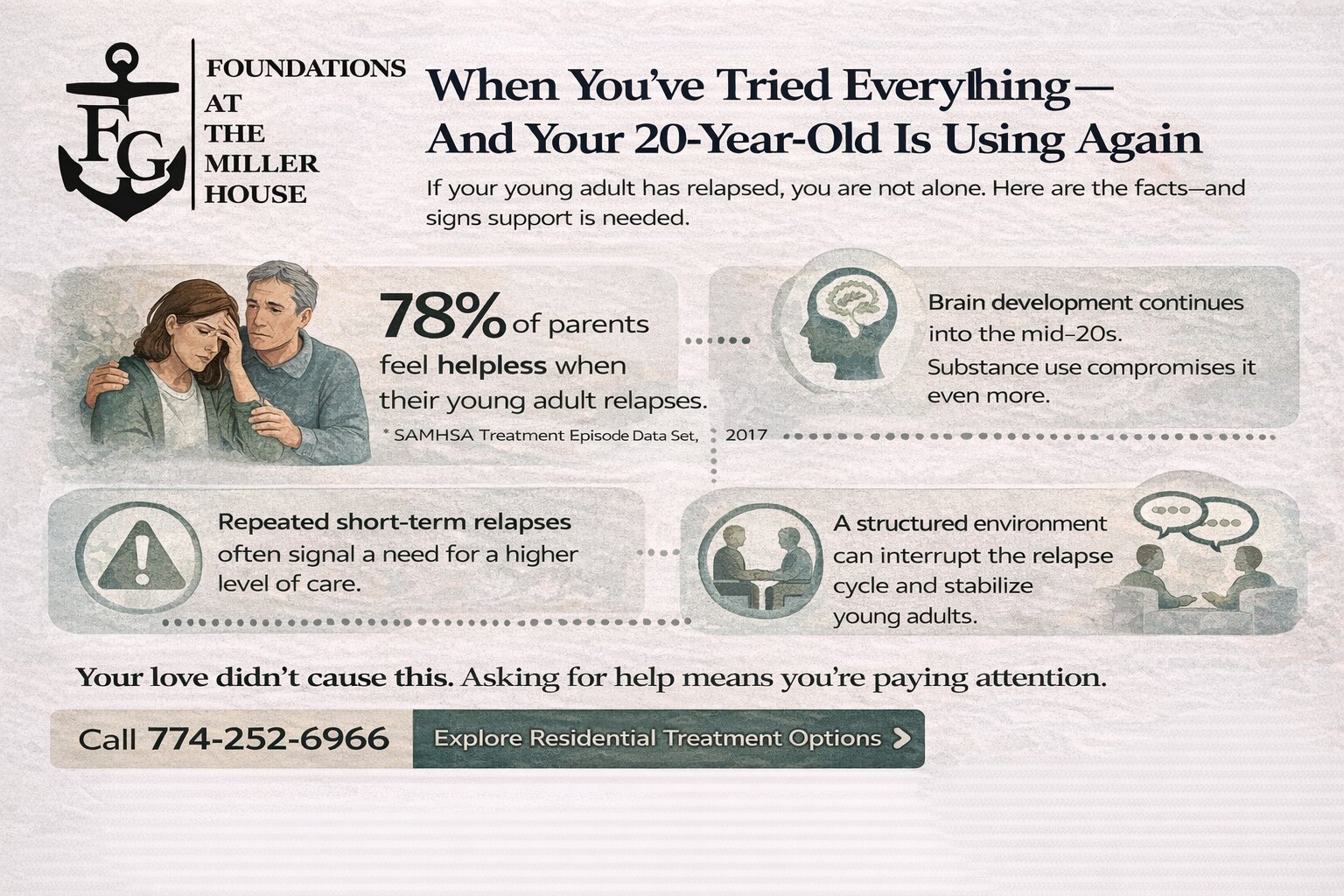
If you’re already exploring options like live-in treatment at Miller House, it’s probably because what you’re doing at home no longer feels sustainable. That doesn’t mean you’ve failed. It means you’re paying attention.
Let’s walk through what this stage often looks like—and what it can become.
The Kind of Grief No One Talks About
When a 20-year-old returns to substance use after progress, parents experience a layered kind of grief.
It’s not just fear for their safety.
It’s the collapse of hope you were quietly rebuilding.
It’s watching independence slip backward.
It’s feeling like you’re bracing for impact all over again.
Many parents tell me they feel embarrassed to even talk about it. As if relapse or continued use reflects poorly on the family.
It doesn’t.
Addiction and mental health struggles are not moral failures. They are complex, biopsychosocial conditions that often require multiple interventions over time. Healing is rarely linear.
But knowing that clinically doesn’t always soothe a parent’s heart.
You may still lie awake thinking, What did I miss? What should I have done differently?
That question alone tells me how deeply you care.
Why Twenty Is More Fragile Than It Looks
On paper, 20 is adulthood.
Neurologically, it isn’t.
The prefrontal cortex—the part of the brain responsible for impulse control, long-term planning, and emotional regulation—continues developing into the mid-20s. Add substances to a still-maturing brain, and decision-making becomes even more compromised.
This is often the age when young adults are:
- Leaving home for the first time
- Managing academic or work pressure
- Navigating adult relationships
- Trying to define who they are
When mental health challenges are layered in—anxiety, depression, trauma—the coping load increases dramatically.
Substance use can begin as relief. Then it becomes escape. Then it becomes entanglement.
Most young adults I work with are not trying to hurt their parents.
They’re trying to quiet something inside themselves they don’t yet know how to manage.
When Home Stops Feeling Like Enough
There’s a moment many parents recognize.
You’re no longer just offering support—you’re monitoring, negotiating, checking phones, tracking behavior, bracing for the next crisis.
You’ve become a case manager in your own home.
That role shift is exhausting. It also strains your relationship.
If your 20-year-old:
- Uses despite clear consequences
- Cannot maintain stability between therapy sessions
- Minimizes serious risks
- Experiences significant mood instability
- Has unsafe peer influences
- Is unable to stay sober in the current environment
It may mean that outpatient therapy or multi-day weekly treatment is not providing enough structure.
And structure isn’t punishment.
It’s containment.
There are times when round-the-clock support creates a pause in the chaos—long enough for deeper work to begin.
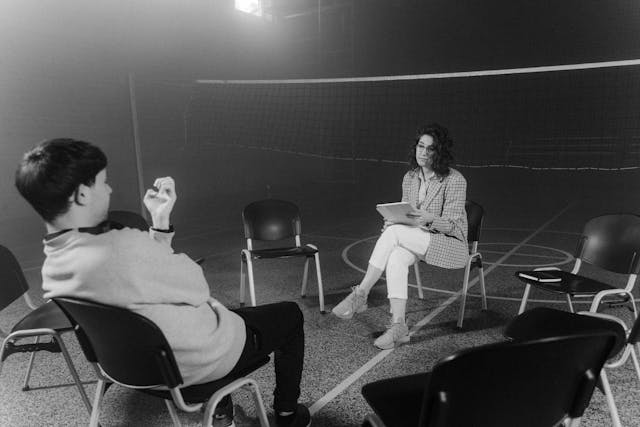
What Actually Happens in a Live-In Setting
Parents often imagine extremes—either overly restrictive environments or something too loose to matter.
In reality, a well-run residential treatment program offers consistency, therapeutic depth, and community.
Here’s what often changes:
1. The Nervous System Settles
Without access to substances and high-risk environments, the body and brain can stabilize. Sleep improves. Appetite normalizes. Emotional reactivity decreases.
Healing requires regulation. Regulation requires safety.
2. Therapy Goes Deeper
In weekly outpatient care, much of the time can be spent stabilizing crises.
In a live-in environment, therapy can explore underlying drivers:
- Trauma
- Attachment wounds
- Identity confusion
- Co-occurring depression or anxiety
- Shame cycles
That depth often isn’t possible when someone is cycling in and out of active use.
3. Parents Step Back into Their Proper Role
This may be the most important shift.
When clinicians hold boundaries and provide accountability, you no longer have to be the enforcer.
You get to be the parent again.
That distinction protects your relationship.
“But They’ve Already Been to Treatment…”
This hesitation is understandable.
If your child has already attended a residential treatment program before, you might think:
If it didn’t work then, why would it work now?
Here’s what I’ve seen over years of practice:
Treatment doesn’t fail because someone struggles afterward. It often plants seeds that take time to grow.
A young adult who resisted therapy at 18 may arrive at 20 with more insight.
What once felt forced can later feel chosen.
What was external pressure can shift into internal motivation.
I’ve watched former clients return with more humility, more honesty, and more readiness.
Growth is developmental. Timing matters.
The Emotional Math Parents Carry
You’re likely weighing things in your head constantly:
- How bad is it really?
- Am I overreacting?
- What if I push too hard?
- What if I don’t push enough?
- What if this damages our relationship?
- What if something terrible happens?
That mental math is exhausting.
Here’s a reframing I often offer:
If the current path is increasing risk and decreasing stability, doing nothing is also a decision.
Choosing a higher level of care is not escalation out of panic—it’s escalation out of care.
Signs a Higher Level of Support May Be Needed
You might consider more intensive live-in care if you notice:
- Repeated cycles of short-term improvement followed by rapid relapse
- Increasing secrecy or isolation
- Legal, academic, or employment consequences stacking up
- Self-harm behaviors or suicidal statements
- Significant untreated trauma
- Extreme mood swings or panic episodes
- Inability to maintain sobriety outside a controlled setting
This isn’t about labeling your child as “severe.”
It’s about matching the intensity of care to the intensity of need.
Hope, Without Fantasy
I want to be honest with you.
No program guarantees permanent sobriety. No environment eliminates risk forever.
What structured care can provide is:
- Stabilization
- Skill-building
- Emotional insight
- Peer accountability
- Clinical evaluation for co-occurring conditions
- A reset in family dynamics
I’ve seen young adults who arrived defensive and withdrawn begin to speak openly about shame they had buried for years.
I’ve watched parents reconnect with their children in family therapy sessions where both sides finally felt heard.
It’s not cinematic transformation.
It’s steady rebuilding.
And steady is enough.
What This Can Become Part of Your Story
One of the most powerful things I’ve witnessed is the way families later describe this chapter.
Not as “the time everything fell apart.”
But as “the time we stopped pretending we could handle it alone.”
Sometimes a residential treatment program becomes a turning point—not because it fixes everything overnight, but because it interrupts a dangerous trajectory.
It creates space.
And in that space, your child can rediscover who they are without substances shaping every decision.
Frequently Asked Questions
How long does live-in care typically last?
Length of stay varies depending on clinical need. Many programs recommend several weeks to a few months to allow for stabilization and meaningful therapeutic work. The goal isn’t speed—it’s sustainable progress.
What if my child refuses to go?
This is common. Young adults often resist higher levels of care. A clinical team can help you explore motivational strategies and family conversations that preserve dignity while maintaining boundaries. Sometimes the shift begins with education, not force.
Will this damage our relationship?
In my experience, the opposite often happens. When professionals hold structure, parents can return to being supportive rather than policing. Family therapy within a live-in setting can strengthen communication and repair trust.
How do we know it’s not “too much”?
Appropriate care is about safety and stabilization, not punishment. If outpatient support has repeatedly failed to hold progress, stepping up care is often proportional—not excessive.
What about school or work?
Programs often coordinate with families to address academic or employment disruptions. While temporary pauses can feel frightening, untreated substance use typically causes greater long-term disruption than a structured pause for healing.
What if they relapse again afterward?
Recovery is not always linear. Even if setbacks occur, skills, insight, and therapeutic relationships gained during structured care often reduce severity and duration of future relapses.
Seeds planted in safety have a way of resurfacing later.
If You’re Standing at the Edge of This Decision
You don’t have to commit to everything today.
You can ask questions.
You can gather information.
You can explore whether a residential treatment program fits your child’s current needs.
What you don’t have to do is carry this alone.
Call (774) 252-6966 or visit our residential treatment program services to learn more about our residential treatment program services in Falmouth, MA.